
Face / Neck Lift
There are multiple face lift techniques available to the Surgeon and the patient and their benefits and virtues are extolled by those that undertake them. Our aim in lifting the face is to give an harmonious look that makes the patient look younger but in a way that minimises the tell tale signs of the surgery. We believe a high SMAS/deep plane face lift is the optimum technique to achieve this.
As a result, the outcome we aim to provide should look natural, younger and brighter and potentially put patients back by 10 to 15 years. We use a technique that not only lifts the neck and jowl but simultaneously also lifts the mid face and cheek through the same incisions as the neck and lower face.
Deep Plane SMAS Face Lift
The technique we use is that of a Deep Plane High SMAS face lift. This is most often in combination with restoring volume of the face by taking fat from the thighs and placing this in areas of volume loss within the face.
This technique has multiple advantages in our opinion over conventional techniques such as a standard deep plane face lift/SMAS plication or the MACS lift/minimal scar face lifts. Its advantage is that it is a face lift that not only rejuvenates the neck and the jowls of the lower face but it also manages to provide a lift to the mid face. This therefore dispenses with a separate mid face lift and the swelling or down time associated with the mid face lifts.
If you are therefore interested in discussing potential treatment with Matthew Potter please contact us here.
Further information regarding face lifting techniques can be found at;
https://www.bapras.org.uk/public/patient-information/surgery-guides/face-and-brow-lift
https://baaps.org.uk/patients/procedures/12/facelift_and_necklift
The cheek descends in time producing folds between the cheek/side of the nose and the corner of the mouth. Elevating this area maintains continuity and harmony from the eye lid down. This procedure is a mid face lift. Conventional mid face lifts are powerful in their results.
They involve incisions in the temple and about the lower eye lid. This allows the surgeon to take the cheek and re-suspend this tissue higher. With time, the mid face looses its volume due to the loss of mid face fat. Mid face lifts however can resuspend a cheek that has lost volume and therefore have little benefit. It may well lie higher but the overlying skin and cheek has no substance.
Our approach to the mid face is to increase the volume of fat within the cheek by taking the patient’s fat from their legs and placing the fat through tiny cannulas into the cheek, the lower eye lid and tear trough. Once the cheek has a restored volume we can then mobilise upwards and outwards through the “High SMAS face lift .”
The facial skin lies on a strong tissue within the cheek called SMAS which descends with time. The SMAS attaches to deeper structures of the facial skeleton through thick bands. These band lie within the cheek. Conventional face lift approaches don’t address these ligaments. This limits their elevation.
The High SMAS lift involves dissecting within the face in front of a gland called the parotid gland. At the front of the gland are strong retaining ligaments. These ligaments once divided allow the SMAS to lift dramatically. It is only by releasing these ligaments can we transfer tension on the SMAS to the jowls as well as elevating the entire cheek tissue.
Our face lift allows us to raise the deeper structures to be independent of the overlying skin. This in effect means a deep tissue elevation but we can replace the skin without any wind swept look or other tell tale signs of a face lift. Our technique provides a smooth contour to the jaw line.
From the lower face to the collar bone, the neck ages through the formation of;
- apparent skin excess,
- tight bands from the underlying platysma muscle and the
- deposition of fat under the jaw line.
Simply pulling the neck tissue upwards as per conventional face lifts won’t necessarily increase the jaw profile or tighten the neck skin and platysma.
The effect of our approach to the platysma is to define the jaw profile as well as tighten the neck skin but also to increase the angle the side of the neck from the jaw line (please refer the before and after photographs).
Bulky tissue under the jaw hinders jaw definition. This tissue relates to fat deposition and the muscles under the jaw line. We reduce this tissue to allow the skin and platysma muscle to tighten against less resistance from the underlying tissue and this therefore give a cleaner jaw profile.
What we describe above is our algorhytm to rejuvenate the face. This approach has evolved over the last 10 years through reviewing results and undertaking discussion with international colleagues reviewing our and their outcomes, patient feedback and above all technique safety.
Share



High SMAS deep plane face lift with lipofill

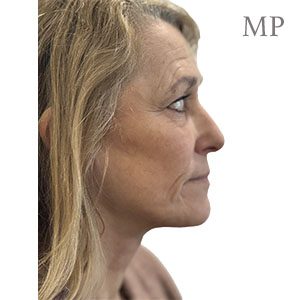
Lipofilling to the; temple, brows, mid face and genio-mandibular groove with a High SMAS, deep plane face lift. Result at 6 months.


Lipofilling to the; temple, brows, mid face and genio-mandibular groove with a High SMAS, deep plane face lift. Result at 6 months.


High SMAS deep plane face lift with lipofill


High SMAS deep plane face lift


High SMAS deep plane face lift with lipofill


High SMAS deep plane face lift anterior profile


High SMAS deep plane face lift lateral profile
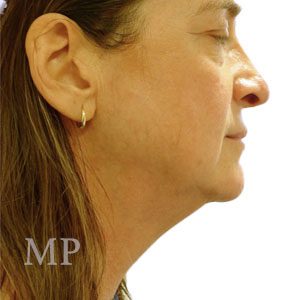

High SMAS deep plane face lift with lipofilling, lateral profile


High SMAS deep plane face lift, anterior profile at 7 weeks


High SMAS deep plane face lift at three months
Number of face lifting procedures undertaken
Greater than 160
Number of years undertaking face lifting procedures
13
Percentage of cases with facial nerve injury post operatively
0%
Unplanned return to theatre
<0.5%
Haematoma
0.5%
Percentage skin loss/slough
0%
Percentage wound healing issues needing dressings
0%
Percentage return to theatre for corrections
0%
Wound break down
0%